|
Chapter 9 : Adult Cardiac Arrest AlgorithmLet’s look at the adult cardiac arrest algorithm and apply it to our scenario from the previous chapter. Please review the scenario. Adult Cardiac Arrest Algorithm Video:Management: Initiate the cardiac arrest algorithm if the patient still has no pulse and does not respond to BLS
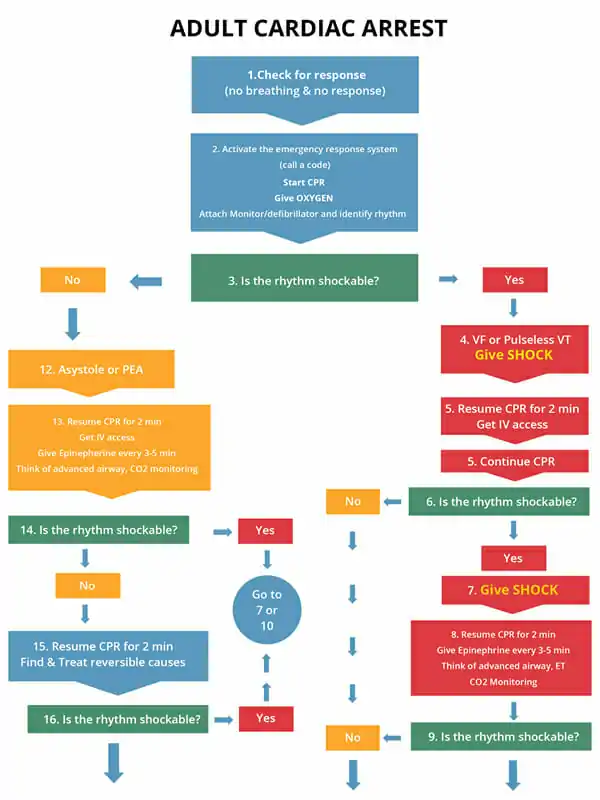
The following algorithm is for Adult Cardiac Arrest:
Treatment of VF/VT in HypothermiaSevere accidental hypothermia in patients with VF and/or VT have a body temperature of <30 degrees Celsius or <86 degrees F. Defibrillation is appropriate in this case, however, additional shocks may need to be given. For those in cardiac arrest with moderate hypothermia (under 36 degrees Celsius), do CPR, defibrillation, give medications, and continue warming the core temperature to raise it above 35 degrees Celsius (95 degrees F). Administration of drugs is usually contraindicated in patients as it may increase levels of toxins due to decreased metabolism. Best treatment for the patient is to focus on raising the core temperature. Administration of vasopressor as per the guidelines of ACLS can be effective while rewarming the patient. Administration of antiarrhythmic drugs is not effective to hypothermic patients. Route of Administration of Drugs in Cardiac ArrestThere are 2 routes of drug administration which are effective and will not interfere with high-quality CPR and defibrillation. These routes are:
The IV route is the most approved route for administrating fluids and medications. The 2 routes are through the peripheral IV line and the central IV line. The IO route is used to inject medication directly into the bone marrow. The IO access can be used in all age groups, but is preferred in pediatric patients. It can be accessed in 30-60 seconds and can be used with any medication that is used in the IV route. Medications used in Cardiac Arrest
Learning Outcomes:You have completed Chapter IX. Now you should be able to:


|
Let’s look at the adult cardiac arrest algorithm and apply it to our scenario from the previous chapter. Please review the scenario.
Management: Initiate the cardiac arrest algorithm if the patient still has no pulse and does not respond to BLS
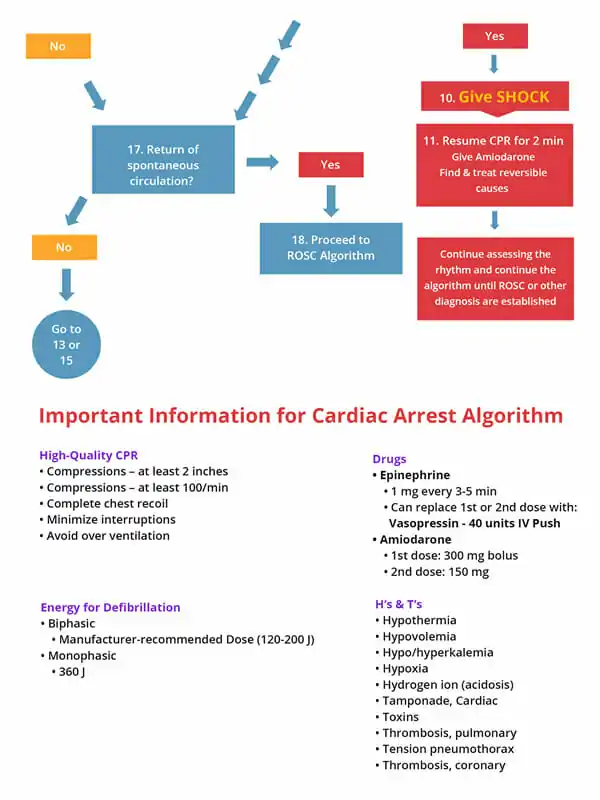
During CPR give the following vasopressors
Administer the following antiarrhythmic drugs after 1st or 2nd dose of epinephrine
The following algorithm is for Adult Cardiac Arrest:
Severe accidental hypothermia in patients with VF and/or VT have a body temperature of <30 degrees Celsius or <86 degrees F. Defibrillation is appropriate in this case, however, additional shocks may need to be given. For those in cardiac arrest with moderate hypothermia (under 36 degrees Celsius), do CPR, defibrillation, give medications, and continue warming the core temperature to raise it above 35 degrees Celsius (95 degrees F).
Administration of drugs is usually contraindicated in patients as it may increase levels of toxins due to decreased metabolism. Best treatment for the patient is to focus on raising the core temperature. Administration of vasopressor as per the guidelines of ACLS can be effective while rewarming the patient. Administration of antiarrhythmic drugs is not effective to hypothermic patients.
There are 2 routes of drug administration which are effective and will not interfere with high-quality CPR and defibrillation. These routes are:
The IV route is the most approved route for administrating fluids and medications. The 2 routes are through the peripheral IV line and the central IV line.
The IO route is used to inject medication directly into the bone marrow. The IO access can be used in all age groups, but is preferred in pediatric patients. It can be accessed in 30-60 seconds and can be used with any medication that is used in the IV route.
Vasopressors
Antiarrhythmic Agents
Amiodarone – given in VF or pulseless V
Lidocaine – consider this if no amiodarone
Magnesium Sulfate – stop recurrent torsades de pointes
You have completed Chapter IX. Now you should be able to: