|
Chapter 15 : Unstable TachycardiaTachycardia is when the heart rate or rhythm is too fast (>100 beats/min). In persistent cases, it can lead to hypotension, acute heart failure, chest pain and possible signs of shock. An increase in heart rate causes less blood to be pumped through the systemic and pulmonary systems. Low blood flow will cause less oxygen to flow to the heart and brain and less oxygen to the heart can lead to Ischemia and MI. Unstable tachycardia is when the heart rate is too fast causing unstable conditions and symptoms caused by >150bpm. Some symptoms may include:
Unstable Tachycardia Video:Unstable Tachycardia Rhythms Include:
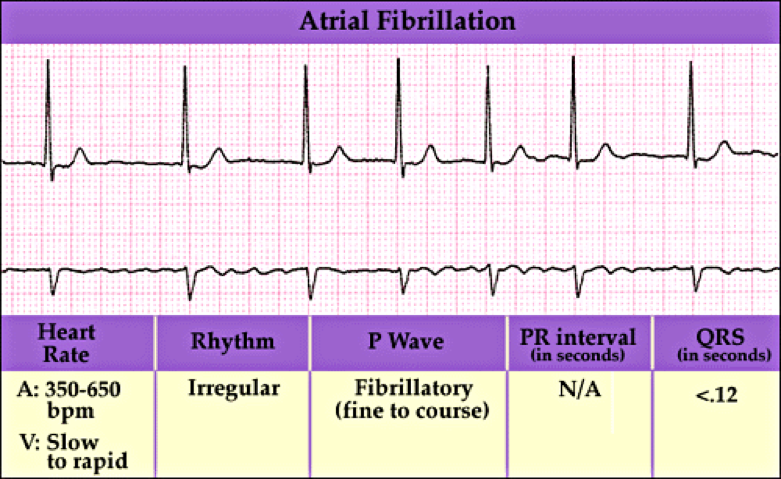
Atrial fibrillation is when the heart beats do not occur at the same intervals. It is known as the quivering of the muscles and involves both the atriums of the heart.
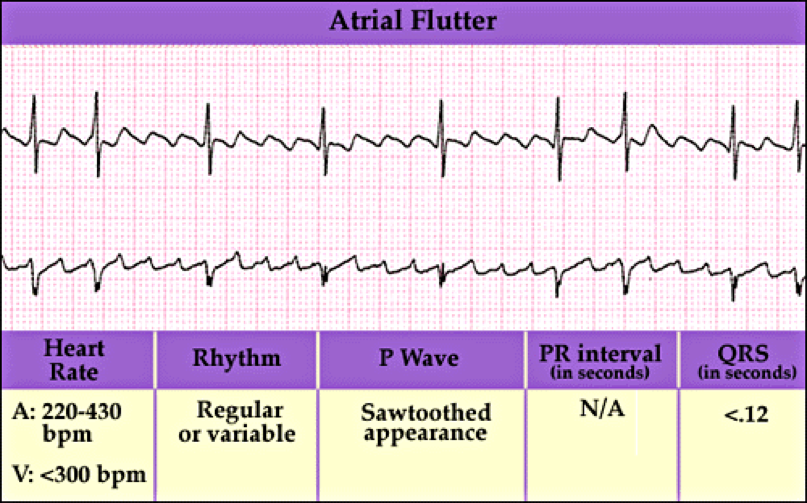
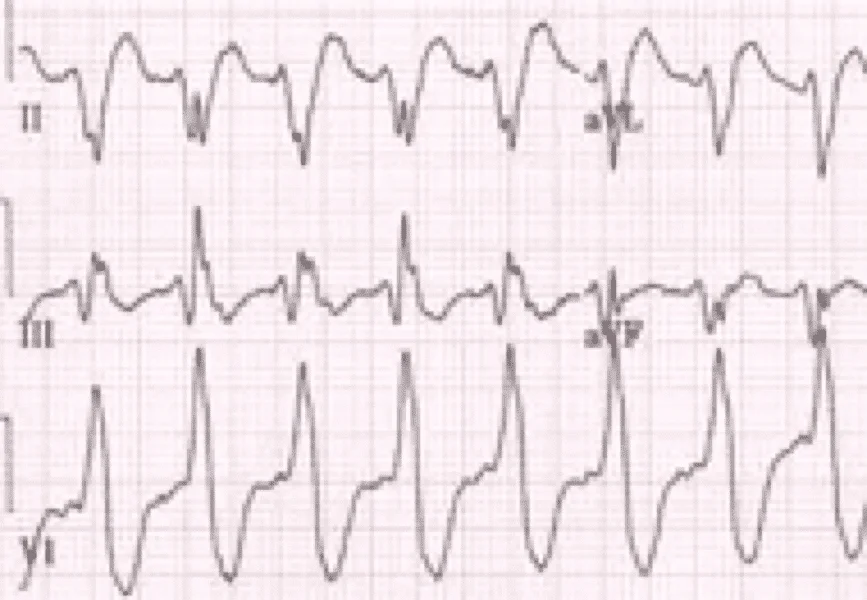
Atrial flutter is abnormal heart rhythm causing fast irregular heartbeat. Starts in the atrium and can lead to atrial fibrillation. Usually has a ‘saw-toothed’ appearance.
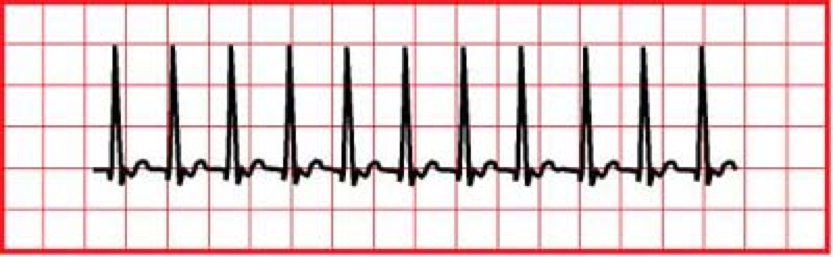
Supraventricular Tachycardia (SVT) is a rapid and narrow heartbeat that starts in the atria or AV node.
Monomorphic VT is heart rate of >150 bpm but all QRS look the same.
Polymorphic VT is when different areas in the ventricles fire fast, uncoordinated impulses.
Wide-complex tachycardia is due to ventricular tachycardia or SVT with wide QRS complex (at least 0.12 seconds).
Scenario: A 45 year old patient arrives to the hospital with chest pain and palpatations. As the nurse was obtaining medical history and checking vital signs the patient faints for a few minutes. Unstable Tachycardia Rhythm Assessment:
Unstable Tachycardia Rhythm Interventions:
Unstable Tachycardia Rhythm Management:
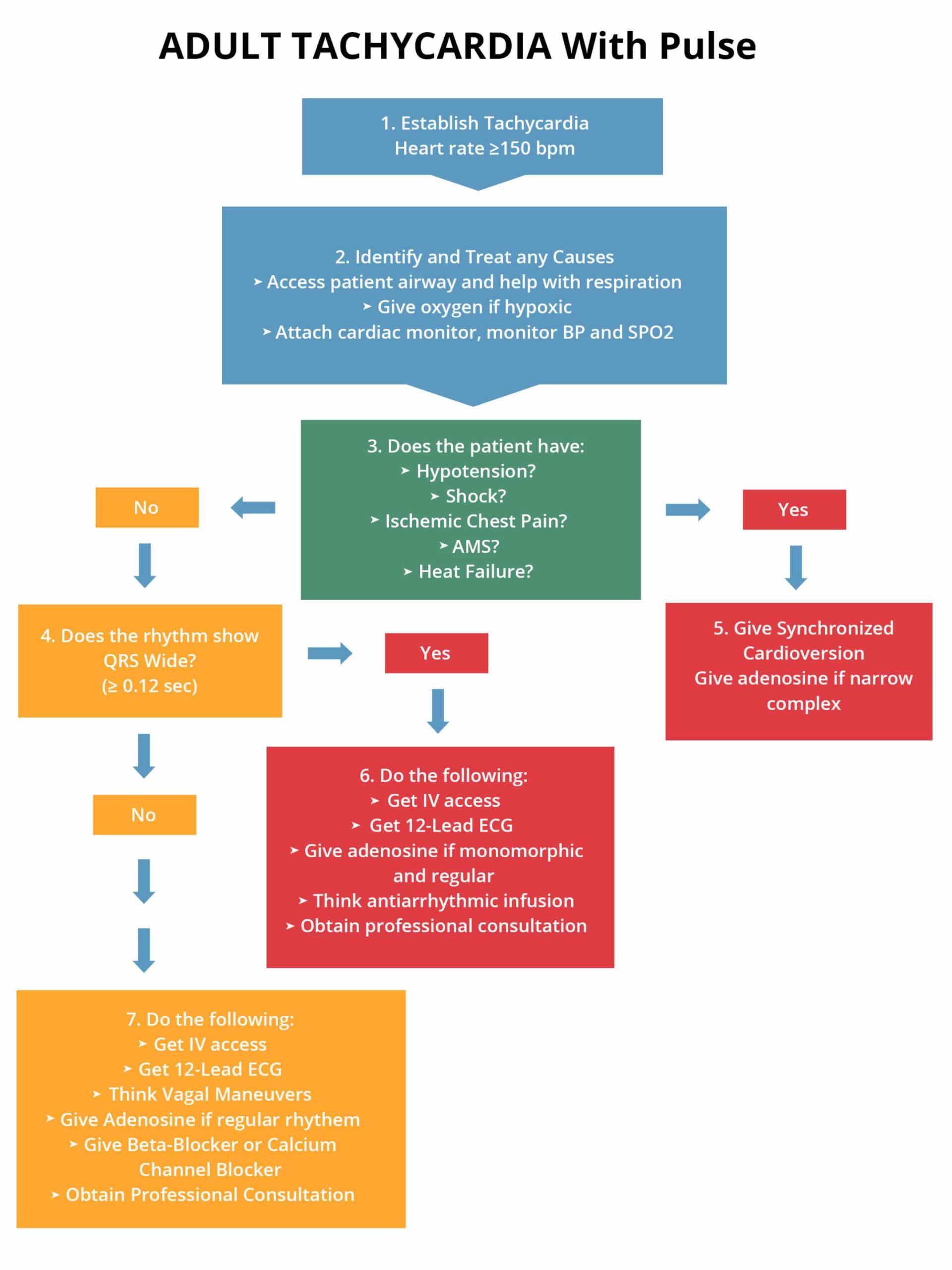
The following is an algorithm showing management of unstable tachycardia in detail:
Cardioversion Synchronized cardioversion is used during unstable tachycardia, but there may be times when unsynchronized cardioversion will need to be used. Synchronized cardioversion needs to be used with:
Unsynchronized cardioversion needs to be used with:
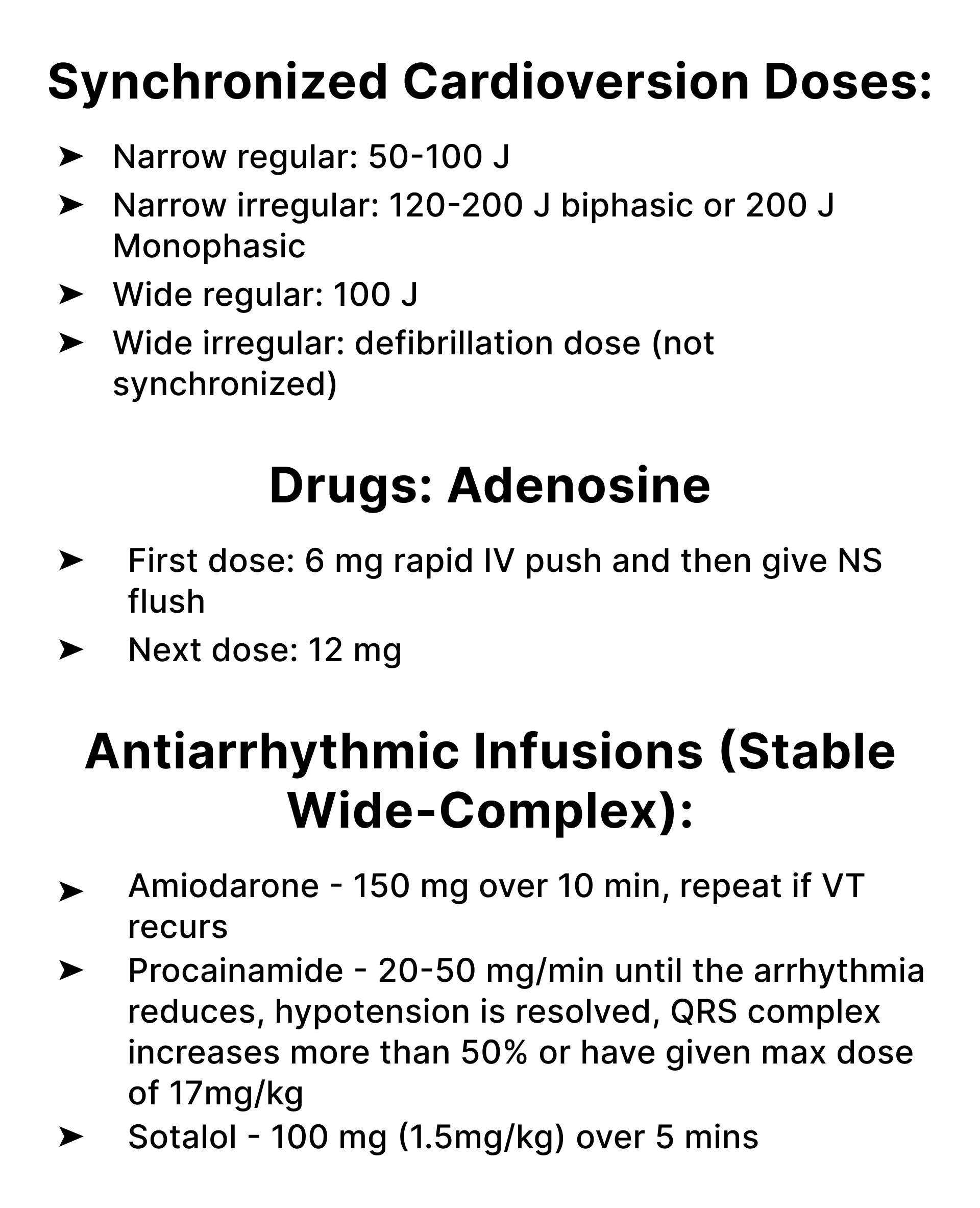
Energy in Joules used during cardioversion:
Learning Outcomes:You have completed Chapter XV. Now you should be able to:


|
||||||||||||
Tachycardia is when the heart rate or rhythm is too fast (>100 beats/min). In persistent cases, it can lead to hypotension, acute heart failure, chest pain and possible signs of shock. An increase in heart rate causes less blood to be pumped through the systemic and pulmonary systems. Low blood flow will cause less oxygen to flow to the heart and brain and less oxygen to the heart can lead to Ischemia and MI. Unstable tachycardia is when the heart rate is too fast causing unstable conditions and symptoms caused by >150bpm. Some symptoms may include:
Atrial fibrillation is when the heart beats do not occur at the same intervals. It is known as the quivering of the muscles and involves both the atriums of the heart.
Atrial flutter is abnormal heart rhythm causing fast irregular heartbeat. Starts in the atrium and can lead to atrial fibrillation. Usually has a ‘saw-toothed’ appearance.
Supraventricular Tachycardia (SVT) is a rapid and narrow heartbeat that starts in the atria or AV node.
Monomorphic VT is heart rate of >150 bpm but all QRS look the same.
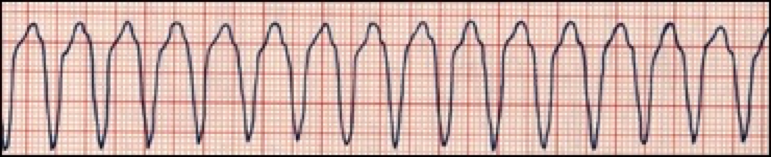
Polymorphic VT is when different areas in the ventricles fire fast, uncoordinated impulses.

Wide-complex tachycardia is due to ventricular tachycardia or SVT with wide QRS complex (at least 0.12 seconds).
Scenario: A 45 year old patient arrives to the hospital with chest pain and palpatations. As the nurse was obtaining medical history and checking vital signs the patient faints for a few minutes.
If persistent tachyarrhythmia initiate synchronized cardioversion
The following is an algorithm showing management of unstable tachycardia in detail:
Cardioversion
Synchronized cardioversion is used during unstable tachycardia, but there may be times when unsynchronized cardioversion will need to be used.
Synchronized cardioversion needs to be used with:
Unsynchronized cardioversion needs to be used with:
Energy in Joules used during cardioversion:
| Rhythm | First Dose (Monophasic Defibrillator) |
| Unstable atrial fibrillation | 200 J |
| Unstable Monomorphic VT | 100 J |
| Other unstable SVT, Atrial Flutter | 200 J |
| Unstable polymorphic VT (irregular form & rate) | Use like VF with high-energy shock (360J) |
| How to Give Synchronized Cardioversion |
|
Anesthetize patient unless they are crashing or unstable
|
You have completed Chapter XV. Now you should be able to: