|
Chapter 14 : Ventricular Fibrillation (VF) & Pulseless Ventricular TachycVentricular fibrillation (VF) is an arrhythmia, which can cause sudden cardiac arrest. During ventricular fibrillation there is no organization of electrical activity in the heart. There is irregular and disarray of cardiac muscle. During VF, blood is not pumped through the systemic or pulmonary circulation leading to irregular heartbeat. VF can change into asystole and sudden cardiac death in a matter of minutes. Ventricular Fibrillation CausesVentricular tachycardia (V-tach or VT) is a fast heart rhythm from the ventricles of the heart. VT can lead to VF and cause sudden death of the patient. A pulseless VT has no cardiac output causing no pulse and results in cardiac arrest. Ventricular fibrillation (VF) is an arrhythmia, which can cause sudden cardiac arrest. During ventricular fibrillation there is irregular organization of electrical activity in the heart. VF causes are listed below.
VF Symptoms
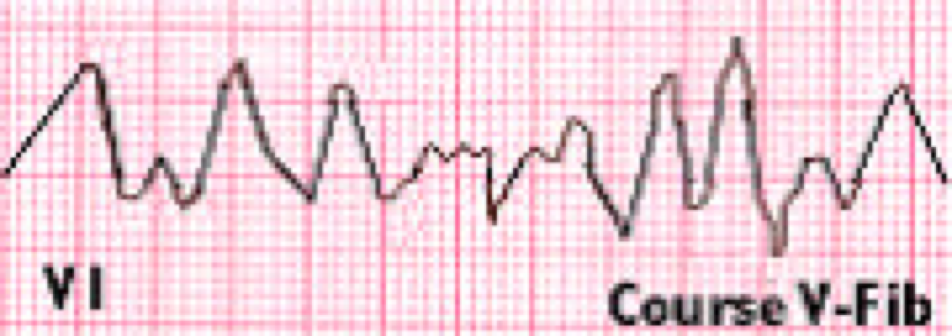
VF does not have an identifiable ECG waveform. Earlier waveforms show a “coarse VF,” but after few minutes the waveforms are much smaller and show a “fine VF.”
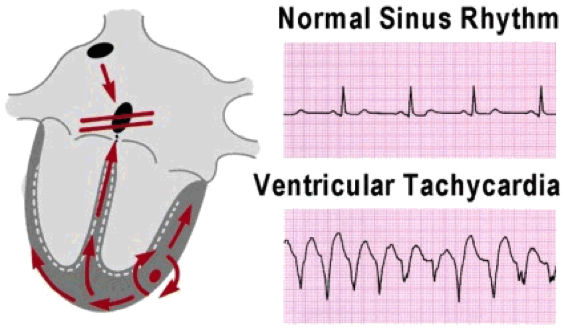
Pulseless Ventricular TachycardiaVentricular tachycardia (V-tach or VT) is a fast heart rhythm from the ventricles of the heart. VT can lead to VF and cause sudden death of the patient. A pulseless VT has no cardiac output causing no pulse and results in cardiac arrest. The causes of pulseless VT are:
The symptoms of pulseless VT are similar to that of VF and follow the same treatment protocol.
This section will cover assessment, intervention, and management of an adult with VF or pulseless VT where the abnormal rhythm is recurrent or did not respond to the first shock. Instead of using the AED, a manual defibrillator will need to be used. The management of VF, pulseless VT, ECG artifact that resembles VF and New left bundle branch block will be covered. Management of these cardiac rhythms will require the efforts of a full team. A resuscitation team includes the following:
Let’s take a look at a scenario. Scenario: You are on-call at the ER and you see a man running towards you and all of a sudden you see him fall to the ground. You rush over there and notice that the man is holding his chest and is having difficulty breathing. After few seconds he loses consciousness. Pulseless Ventricular Tachycardia Assessment
Pulseless Ventricular Tachycardia Interventions
Pulseless Ventricular Tachycardia ManagementInitiate the cardiac arrest algorithm if the patient still has no pulse and does not respond to BLS. We will look at the Cardiac Arrest Algorithm in the following chapter. Learning Outcomes:You have completed Chapter VIII. Now you should be able to:


|
Ventricular fibrillation (VF) is an arrhythmia, which can cause sudden cardiac arrest. During ventricular fibrillation there is no organization of electrical activity in the heart. There is irregular and disarray of cardiac muscle. During VF, blood is not pumped through the systemic or pulmonary circulation leading to irregular heartbeat. VF can change into asystole and sudden cardiac death in a matter of minutes.
Ventricular tachycardia (V-tach or VT) is a fast heart rhythm from the ventricles of the heart. VT can lead to VF and cause sudden death of the patient. A pulseless VT has no cardiac output causing no pulse and results in cardiac arrest. Ventricular fibrillation (VF) is an arrhythmia, which can cause sudden cardiac arrest. During ventricular fibrillation there is irregular organization of electrical activity in the heart. VF causes are listed below.
VF does not have an identifiable ECG waveform. Earlier waveforms show a “coarse VF,” but after few minutes the waveforms are much smaller and show a “fine VF.”
Ventricular tachycardia (V-tach or VT) is a fast heart rhythm from the ventricles of the heart. VT can lead to VF and cause sudden death of the patient. A pulseless VT has no cardiac output causing no pulse and results in cardiac arrest. The causes of pulseless VT are:
The symptoms of pulseless VT are similar to that of VF and follow the same treatment protocol.
This section will cover assessment, intervention, and management of an adult with VF or pulseless VT where the abnormal rhythm is recurrent or did not respond to the first shock. Instead of using the AED, a manual defibrillator will need to be used. The management of VF, pulseless VT, ECG artifact that resembles VF and New left bundle branch block will be covered. Management of these cardiac rhythms will require the efforts of a full team.
A resuscitation team includes the following:
Let’s take a look at a scenario.
Scenario: You are on-call at the ER and you see a man running towards you and all of a sudden you see him fall to the ground. You rush over there and notice that the man is holding his chest and is having difficulty breathing. After few seconds he loses consciousness.
Initiate the cardiac arrest algorithm if the patient still has no pulse and does not respond to BLS.
We will look at the Cardiac Arrest Algorithm in the following chapter.
You have completed Chapter VIII. Now you should be able to: